Privacy Policy for Sono
Last updated: March 28, 2021
This Privacy Policy describes Our policies and procedures on the collection, use and disclosure of Your information when You use the Service and tells You about Your privacy rights and how the law protects You.
We use Your Personal data to provide and improve the Service. By using the Service, You agree to the collection and use of information in accordance with this Privacy Policy. This Privacy Policy has been created with the help of the Privacy Policy Generator.
Interpretation and Definitions
Interpretation
The words of which the initial letter is capitalized have meanings defined under the following conditions. The following definitions shall have the same meaning regardless of whether they appear in singular or in plural.
Definitions
For the purposes of this Privacy Policy:
- Account means a unique account created for You to access our Service or parts of our Service.
- Affiliate means an entity that controls, is controlled by or is under common control with a party, where “control” means ownership of 50% or more of the shares, equity interest or other securities entitled to vote for election of directors or other managing authority.
- Application means the software program provided by the Company downloaded by You on any electronic device, named Sono
- Company (referred to as either “the Company”, “We”, “Us” or “Our” in this Agreement) refers to Sono.
- Country refers to: Ontario, Canada
- Device means any device that can access the Service such as a computer, a cellphone or a digital tablet.
- Personal Data is any information that relates to an identified or identifiable individual.
- Service refers to the Application.
- Service Provider means any natural or legal person who processes the data on behalf of the Company. It refers to third-party companies or individuals employed by the Company to facilitate the Service, to provide the Service on behalf of the Company, to perform services related to the Service or to assist the Company in analyzing how the Service is used.
- Third-party Social Media Service refers to any website or any social network website through which a User can log in or create an account to use the Service.
- Usage Data refers to data collected automatically, either generated by the use of the Service or from the Service infrastructure itself (for example, the duration of a page visit).
- You means the individual accessing or using the Service, or the company, or other legal entity on behalf of which such individual is accessing or using the Service, as applicable.
Collecting and Using Your Personal Data
Types of Data Collected
Personal Data
We do not collect any data that can be linked to You, or be used to identify You.
Device ID Data
When You access the Service by or through a mobile device, We may collect certain information automatically, including, but not limited to, the type of mobile device You use, Your mobile device unique ID, the IP address of Your mobile device, Your mobile operating system, the type of mobile Internet browser You use, unique device identifiers and other diagnostic data.
Use of Your Personal Data
The Company may use Personal Data for the following purposes:
- To provide and maintain our Service, including to monitor the usage of our Service.
- To manage Your Account: to manage Your registration as a user of the Service. The Personal Data You provide can give You access to different functionalities of the Service that are available to You as a registered user.
- For the performance of a contract: the development, compliance and undertaking of the purchase contract for the products, items or services You have purchased or of any other contract with Us through the Service.
- For other purposes: We may use Your information for other purposes, such as data analysis, identifying usage trends, determining the effectiveness of our promotional campaigns and to evaluate and improve our Service, products, services, marketing and your experience.
We may share Your personal information in the following situations:
- With Service Providers: We may share Your personal information with Service Providers to monitor and analyze the use of our Service, to contact You.
- For business transfers: We may share or transfer Your personal information in connection with, or during negotiations of, any merger, sale of Company assets, financing, or acquisition of all or a portion of Our business to another company.
- With Affiliates: We may share Your information with Our affiliates, in which case we will require those affiliates to honor this Privacy Policy. Affiliates include Our parent company and any other subsidiaries, joint venture partners or other companies that We control or that are under common control with Us.
- With business partners: We may share Your information with Our business partners to offer You certain products, services or promotions.
- With Your consent: We may disclose Your personal information for any other purpose with Your consent.
Retention of Your Personal Data
The Company will retain Your Personal Data only for as long as is necessary for the purposes set out in this Privacy Policy. We will retain and use Your Personal Data to the extent necessary to comply with our legal obligations (for example, if we are required to retain your data to comply with applicable laws), resolve disputes, and enforce our legal agreements and policies.
The Company will also retain Usage Data for internal analysis purposes. Usage Data is generally retained for a shorter period of time, except when this data is used to strengthen the security or to improve the functionality of Our Service, or We are legally obligated to retain this data for longer time periods.
Transfer of Your Personal Data
Your information, including Personal Data, is processed at the Company’s operating offices and in any other places where the parties involved in the processing are located. It means that this information may be transferred to — and maintained on — computers located outside of Your state, province, country or other governmental jurisdiction where the data protection laws may differ than those from Your jurisdiction.
Your consent to this Privacy Policy followed by Your submission of such information represents Your agreement to that transfer.
The Company will take all steps reasonably necessary to ensure that Your data is treated securely and in accordance with this Privacy Policy and no transfer of Your Personal Data will take place to an organization or a country unless there are adequate controls in place including the security of Your data and other personal information.
Disclosure of Your Personal Data
Business Transactions
If the Company is involved in a merger, acquisition or asset sale, Your Personal Data may be transferred. We will provide notice before Your Personal Data is transferred and becomes subject to a different Privacy Policy.
Law enforcement
Under certain circumstances, the Company may be required to disclose Your Personal Data if required to do so by law or in response to valid requests by public authorities (e.g. a court or a government agency).
Other legal requirements
The Company may disclose Your Personal Data in the good faith belief that such action is necessary to:
- Comply with a legal obligation
- Protect and defend the rights or property of the Company
- Prevent or investigate possible wrongdoing in connection with the Service
- Protect the personal safety of Users of the Service or the public
- Protect against legal liability
Security of Your Personal Data
The security of Your Personal Data is important to Us, but remember that no method of transmission over the Internet, or method of electronic storage is 100% secure. While We strive to use commercially acceptable means to protect Your Personal Data, We cannot guarantee its absolute security.
Children’s Privacy
Our Service does not address anyone under the age of 13. We do not knowingly collect personally identifiable information from anyone under the age of 13. If You are a parent or guardian and You are aware that Your child has provided Us with Personal Data, please contact Us. If We become aware that We have collected Personal Data from anyone under the age of 13 without verification of parental consent, We take steps to remove that information from Our servers.
If We need to rely on consent as a legal basis for processing Your information and Your country requires consent from a parent, We may require Your parent’s consent before We collect and use that information.
Links to Other Websites
Our Service may contain links to other websites that are not operated by Us. If You click on a third party link, You will be directed to that third party’s site. We strongly advise You to review the Privacy Policy of every site You visit.
We have no control over and assume no responsibility for the content, privacy policies or practices of any third party sites or services.
Changes to this Privacy Policy
We may update Our Privacy Policy from time to time. We will notify You of any changes by posting the new Privacy Policy on this page.
We will let You know via email and/or a prominent notice on Our Service, prior to the change becoming effective and update the “Last updated” date at the top of this Privacy Policy.
You are advised to review this Privacy Policy periodically for any changes. Changes to this Privacy Policy are effective when they are posted on this page.
Contact Us
If you have any questions about this Privacy Policy, You can contact us:
- By email: [email protected]
- By visiting this page on our website: https://westernsono.ca/sono-privacy-policy/
Introduction to Transesophageal Echocardiography
Dr. Rob Arntfield, MD, FRCPC, gives us a comprehensive introduction to TEE, its indications, its scope, the pros and the cons and considerations for implementing the modality into your practice and/or program. Learn about why TEE isn’t as intimidating as you think and how this could be a cornerstone in the resuscitation of the critically ill patient! This talk was given as a part of the MTL-SONO virtual conference in November 2020.
Role of POCUS DVT studies in different specialties, humbling moment in POCUS, renal TEE!
We have another great episode for you guys! Today we discuss the role of DVT studies in different medical specialties. We then move on to discuss a humbling moment in point-of-care echocardiography which highlights the different roles of POCUS on the one hand and comprehensive cardiac echocardiography on the other. Finally, we have an innovative surprise for you, an unusual assessment of the kidney with point-of-care TEE!
Tune in to listen to the discussion between Dr Robert Arntfield, Dr Jason Lam, Dr Melanie Lemay, Dr Mathilde Gaudreau-Simard and for his last appearance on the show our outgoing CCUS fellow, Dr. Thamer Alaifan
For questions, comments or feedback, please email us at [email protected]
Post-production by Hubert Gaudreau-Simard
Multimedia support by Brian Park, Meds 2023
Music: Nightchaser by Shane Ivers – https://www.silvermansound.com
Clips
Clip 1: WesternSono Screencast on conducting a DVT study
Clip 2: Humbling moment in POCUS; can you spot the anomaly on the aortic valve?
Clip 3: Innovation in POCUS; renal assessment through TEE
Role of Point of care TEE for prosthetic valves, pleural effusion or ascites and the pulsatility index in transcranial doppler
In this episode, we start by taking you through our take on the role of point of care TEE for prosthetic valves. We then discuss a case where looking beyond the pleura was important in identifying large volume ascites causing restriction of diaphragmatic excursion. Finally we touch on transcranial doppler and the pulsatility index. Tune in to listen to the discussion between Dr Robert Arntfield, Dr. Thamer Alaifan, Dr Mathilde Gaudreau-Simard and Dr Jag Brar.
For questions, comments or feedback, please email us at [email protected]
Post-production by Hubert Gaudreau-Simard
Multimedia support by Brian Park, Meds 2023
Music: Nightchaser by Shane Ivers – https://www.silvermansound.com
Clips
Clip 1: Bioprosthetic aortic valve in deep transgastric TEE view
Clip 2: Large volume ascites rather than pleural effusion likely responsible for restrictive respiratory failure
Critical Care Ultrasound Fellows
Current Fellows
Alex is a practicing Intensivist in Winnipeg, having completed medical school and an Internal Medicine residency at Queen’s University, followed by a Critical Care fellowship at the University of Manitoba. He was introduced to POCUS early in his career and gravitated to it to better connect with and understand his patients and their bodies. With a longstanding interest in Medical Education, he joined Western Sono for a Critical Care Ultrasound fellowship in 2022 to deepen his knowledge and expertise in the field. He has been known to bike everywhere, even in winter. Outside the hospital he loves to take off into the backcountry to hike, to ski, or go camping.


Erica, a proud east coaster from Newfoundland, studied medicine at The University of Queensland in Australia. She completed her core Internal Medicine residency at Queen’s University and went on to complete a fellowship in Critical Care Medicine at the University of Manitoba. Her husband and loyal golden retriever, Sally, have followed her across the world and back to support her never ending pursuit of education.
Her interests include ultrasound curriculum development, medical education, gender equity in acute care medicine and resident wellness. In keeping with the theme of sound and harmonics, Erica has a musical past life as a singer-songwriter and, while in medical school, she produced a self-funded album titled Follow Your Dreams. She is now chasing her dream of completing a CCUS fellowship under the directorship of Dr. Robert Arntfield at Western University. Her goal is to inspire and educate acute care clinicians to incorporate CCUS in their clinical practice, raising the standard of care for the diagnosis and management of critical illness
Past Fellows

Apart from being the first U.S trained fellow to venture across the border to join our fellowship Michael is also the first pediatric trained fellow to join the program. Michael completed a combined Internal Medicine-Pediatrics residency program at the University of Illinois, Peoria, and completed his pediatric critical care training at Phoenix Children’s Hospital. He is currently in Blantyre, Malawi as part of a Pediatric Critical Care Global Health Fellowship where he is involved in ultrasound related research.
Michael is originally from Nicaragua, where he hopes to one day help develop a pediatric critical care ultrasound program. Outside of critical care medicine and global health, he is a practitioner of the Afro-Brazilian art form Capoeira Angola. He also enjoys traveling with his wife and two children.
Favorite POCUS experience: Performing TEE and TCD to assist and help guide resuscitation efforts in the trauma bay. Additionally, I truly enjoyed the invaluable career development sessions with Dr. Rob Arntfield and the camaraderie with the other fellows and learners. Shout out to Juan and Ross!
Jason completed his medical school at McMaster University followed by his core Internal Medicine Residency and Critical Care Fellowship at Western University. His fascination with POCUS emerged during his critical care training while learning to use Transesophageal Echocardiography and TELUS in acute resuscitation. This continued to grow during his CCUS fellowship and the pandemic under the guidance of Dr. Robert Arntfield, honing his skills in the management of complex hemodynamics.
Outside of Critical Care Medicine Jason also has an interest in Healthcare Quality Improvement and is currently enrolled in the University of Toronto Master of Science in Quality Improvement and Patient Safety. In his free time Jason enjoys travelling around the world and is always on the move. He is continuing his academic pursuits this year in Auckland, New Zealand in the Cardiovascular Intensive Care and ECMO program.
Favorite POCUS Experience: Using TCDs during acute resuscitation to confirm cerebral perfusion and consequently using TEE to help guide ECMO cannulation.


Zain completed his Internal Medicine Residency and General Internal Medicine Fellowship at Western University. He was first drawn to POCUS when he unwittingly identified blood in the pericardium of a patient admitted with a query STEMI who turned out to have an aortic dissection. From that moment onward he would try and use ultrasound any chance he had (albeit without much skill or knowledge). During his GIM fellowship he had the opportunity to do an ultrasound elective in the ICU under Dr. Robert Arntfield. That experience was transformative as it reinforced his passion for ultrasound and led him to pursue a fellowship in acute care ultrasound. That journey allowed him to develop the tools he needed to become a skilled practitioner and spread the “Gospel of Arntfield” to all the other loyal disciples of ultrasound. When Zain isn’t actively participating in ultrasound education – you can find him outdoors either hiking, kayaking, spending time at the cottage or traveling the world.
Mike completed his core internal medicine residency and General Internal Medicine fellowship at Western University. His fascination with POCUS began during his first elective in CCUS during residency, and blossomed into a vocation under further guidance by Dr. Thamer Alaifan and Dr. Robert Arntfield. Mike’s passions within POCUS are varied and include “putting Doppler on everything”, as well as curating a pristine archive of the best scans he has encountered. Outside of medicine, you can usually find him cooking or enjoying a delicious meal with his family and friends.
Favourite POCUS experience: Having the privilege to spend every Friday afternoon learning, laughing, and eating in the company of like-minded individuals. Image review in the UltraLounge was where every great case could be discussed, acquisition could be critiqued, and POCUS knowledge could be disseminated in ways that made it the highlight of my week on a regular basis.


Melanie completed her General Internal Medicine at Western University. Prior to that, she did her residency at University of Ottawa in her home town. It was here where she first became interested in point of care ultrasound when she saw it being used with a water bath to help diagnose the cause of a sickle cell patient’s joint pain. From there on her POCUS interests grew to whole body ultrasound and she loves learning new applications. She is now developing her own ultrasound program at the Montfort Hospital and recently launched the YouTube channel “POCUS In Practice” with co-fellow Drew!
Favorite POCUS experience: discovering the RIMP…and hanging out in the Ultralounge, scanning each other to teach each other new aspects of ultrasound
Mathilde is a PGY-5 in General Internal Medicine at the University of Ottawa. Mathilde completed medical school and her core medicine training in Montreal at McGill University before crossing over to Ottawa. Her first exposure to POCUS was at McGill in medical school where she saw the very beginnings of the UGME POCUS program. She has since continued to be fascinated with the application of POCUS in medicine and more specifically in Internal Medicine. Fun facts about Mathilde, she holds a law degree from a life before medicine, and bikes everywhere, a habit that she picked up growing up in Tokyo.Favorite POCUS moment; first transcranial doppler where she realized that flow CAN actually be seen through the skull! Find her on twitter @MathildeGSimard for more favorite moments!


Bader received his medical education and training in Saudi Arabia, at the King Saud University in Riyadh. Afterwards, he went on to receive a Master’s Degree in Public Health at the University of Miami. His main interest is in medical education, and he hopes to one day go back to Saudi Arabia to establish a critical care ultrasound program.
Matt grew up in Nova Scotia before heading to Ontario in 2003. He completed his MSc. in Physical Chemistry in 2009 before switching gears and entering the world of medicine. Matt completed his residency in Emergency Medicine and Fellowship in Critical Care at Queen’s University before joining Western for the Critical Care Ultrasound Fellowship. Outside of medicine, Matt can be found training for the odd triathlon, or struggling through a round of golf.


Marko completed four years of internal medicine residency at Dalhousie University in Halifax, NS in 2017 and is currently a PGY6 critical care resident also at Dalhousie. His POCUS interests include diastology and the role of POCUS in patients weaning from mechanical ventilation. Other clinical interests include critical thinking and diagnostic error, mechanical ventilation and quality improvement. He is a novice “tweeter” and enjoys disconnecting and camping anywhere across Canada.
Favourite POCUS experience: Having a patient with prolonged vent wean, write “seeing is believing” on his communication board to me, after I led a bedside lung POCUS teaching session with him.
Katie is a 5th-year fellow in General Internal Medicine from the University of British Columbia. She is spending a year doing POCUS training, of which 6 months are here at Western in the role of CCUS fellow. Follow her on Twitter for cool ultrasound clips and more at @katiewiskar.
Favourite POCUS experience: Nerding out over POCUS clips every Friday afternoon in the Ultralounge. Where else can you spend 3 hours talking about hepatic doppler or dynamic LVOT obstruction?


Dany is from a small town in rural northern Québec and trained in General Internal Medicine at the Université de Sherbrooke. Caring for people in remote northern communities and managing patients crashing in the middle of the night demonstrated that resources are often scarce – and that point of care ultrasound is key to better patient care. Naturally, he migrated west to the mecca of POCUS teaching and education at Western University where he completed his Critical Care Medicine residency, as well as a fellowship in Critical Care Ultrasound. Dany now practices Critical Care and Internal Medicine at the Hôpital Charles-Lemoyne in Longueil, Québec, where he also teaches point of care ultrasound.
Favourite POCUS Experience: 5am in MSICU. New patient, he’s dying… Transferring doc says pneumonia but it doesn’t fit. His vitals – crap; his lungs – white. Time to turn to the probe. His mitral valve is flail! We can fix this! He’s going to live! That’s when I saw POCUS could save a life.
Hailey completed her medical school at NOSM in 2012, followed by internal medicine at Dalhousie University and Critical Care medicine at Western University in London. In addition to POCUS, she has an interest in healthcare quality improvement and is currently enrolled in Queen’s Universities Master of Science in Healthcare Quality and Patient Safety. Hailey is presently working in Kingston, Ontario in the Department of Critical Care Medicine.
Favorite POCUS Experience: The banter at the Friday image review sessions was always a highlight of the week, but two of her most memorable POCUS experiences were performing an endoscopy-guided TEE with Dr. Fortin, and trialling new POCUS techniques like esophageal ultrasound for NG placement, or TELUS.


Dr. Lau received his honors BSc from the University of Toronto, medical degree from the University of British Columbia, and completed his internal medicine residency at the University of Alberta before coming to Western for his Critical Care Fellowship. His special interests are educating people on the importance of critical care and resuscitation medicine, as well as to the uses of advanced point-of-care ultrasound applications. He also enjoys research in the fields of system flow optimization and cost-savings analysis.
Favorite POCUS Experience: My favorite experience in POCUS was training in “whole body ultrasound” (advanced TEE/TEE, lung, vascular: DVT, carotid, venous access, abdominal: renal/hepatic/biliary/aorta/OB/GYN/FF, MSK, head/neck/airway) and the opportunity to research and publish on transcranial Doppler ultrasound. Becoming a testamur/diplomate of the National Board of Echocardiography (Examination of Special Competance in Critical Care Echocardiography) was also an amazing POCUS achievement.
Dr. Brian Buchanan graduated from the University of Alberta with a BSc (hon) in Human Physiology in 2006 and MD in 2010. He went on to complete training in Internal Medicine (Dalhousie University, 2014) and Critical Care Medicine (McMaster University, 2016). Additionally, Brian completed concurrent training in critical care ultrasound and echocardiography (Western University, 2016). He is completing a Masters of Medical Education (Dundee University) with a focus on training, competency and quality assurance in critical care ultrasound (CCUS). Brian was hired by the University of Alberta in 2016 as a faculty intensivist in the Department of Critical Care Medicine. He also began the role of flight physician with the Shock Trauma Air Rescue Society (STARS) in May 2017. His main research interests are curriculum design and ultrasound education and has been leading an Edmonton-wide initiative in CCUS, titles the “ABaCCUS” project (www.ABaCCUS.ca).
Favorite POCUS Experience: Not so much a favorite ultrasound experience as it was serendipitous opportunity. I had just finished completing training in internal medicine and had started in critical care medicine at McMaster University. I had taken a few unconventional electives in IM, which permitted me to set aside ~6 months of time from my ICU fellowship to take on an additional focused competency. I had met Rob at the annual CRUS conference and was immediately awe-struck by the entire experience. Although I came with some prior echo experience, CRUS started the split that tore a hole in my conceptualization of clinical examination. Also….Dr. Arntfield. A consummate professional and a uniquely skilled individual—a personality that wields a strong gravitational field. After some back and forth between Rob and my program director at that time, we decided that we could make this CCUS fellowship happen. To my surprise, the ensuing training and support would indelibly shape my career in ways I could not have imagined.

Hi everyone,
Happy 2020! Hope everyone had a great holiday! It’s great to be back at it with more great cases!
The Case
This is a 74yo F with a past medical history significant for ESRD and severe PVD who was transferred to the ICU overnight with presumed septic shock thought to be related to left foot osteomyelitis. She had presented to the ED with refractory hypotension and altered LOC necessitating intubation and high dose vasopressors. The POCUS team went to do a focused cardiac exam, primarily to see if there was a cardiogenic component to his shock. The following TTE images were taken and the decision was made to perform a point-of-care TEE. What do you think is going on?
TTE Views
TEE Views
The TTE images clearly demonstrate a grossly abnormal mitral valve, but it’s hard to delineate exactly what’s going on. Dialysis patients (as this patient was) are often predisposed to significant mitral valve annular calcification (MAC). When initially assessing this valve, it was difficult to confidently distinguish between severe MAC and potential endocarditis (although highly suspicious for this).
Luckily, we have ready access to a TEE probe, so we quickly made the decision to have a closer look at the valve with TEE. As you can see from those images, the MV pathology is much better delineated and we can assess the MV (and its various scallops) using different omniplane angles. Now we can see a large, independently mobile, hyperechoic lesion primarily on the posterior mitral valve leaflet (although there also looks like there may be some smaller lesions on the AMVL as well). Finally, you might also have noticed a few lesions on the NCC of the aortic valve. Given the pathology evident on the MV, these would also be highly suspicious for AV endocarditis as well (although could also represent calcification).
In the end this patient would grow MRSA in her blood which ultimately would have prompted the team to order an echocardiogram to look for endocarditis. But, using POCUS TEE the patient’s endocarditis was diagnosed more promptly which gave the treating team more diagnostic confidence, avoided chasing other potential diagnoses, and facilitated expedited consultation and management with the appropriate services.
Hi everyone,
Thought we would take a break from the world of echo this week and again illustrate how we are using transcranial doppler in the ICU at Western.
The Case
This is a case of a 52 yo F trauma patient with severe traumatic brain injury. She was intubated and transferred to the ICU where, given the severity of her TBI, an intraparenchymal ICP monitor was placed by neurosurgery. The ICP monitor was initially showing an ICP of 10. Overnight, however, despite no apparent clinical change, the ICP waveform was inconsistent and the readings were now showing values around 40-50. We thus performed a point-of-care TCD to help determine whether her ICP was truly elevated or whether the ICP monitor was giving spurious information. Have a look at the following images. Do you think the TCD spectral waveform is consistent with markedly elevated ICP?
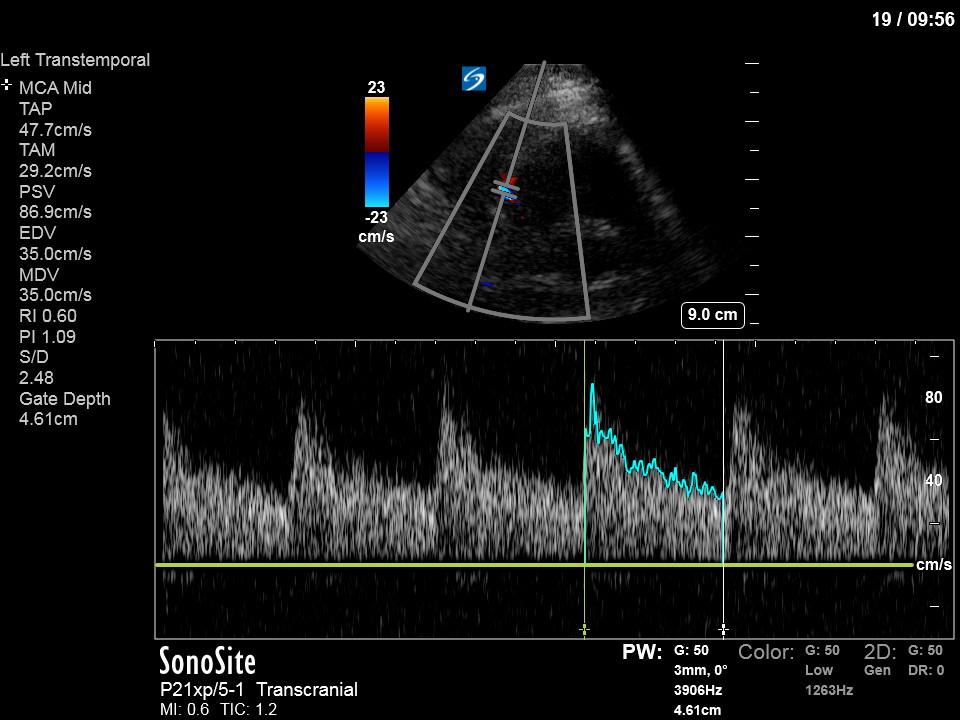
The above images show pulse wave doppler interrogation of the left MCA artery. This produced the typical spectral Doppler velocity waveform with a steep systolic upstroke and the gradual step-down diastolic flow. This is the expected appearance of flow in the absence of raised intracranial pressure.
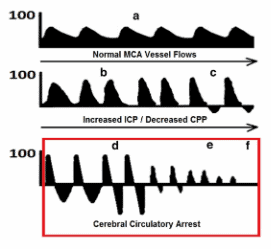
In the setting of raised ICP the diastolic flow becomes blunted, and can even progress to diastolic flow reversal followed by the gradual reduction of systolic flow as the ICP progressively increases towards cerebral circulatory arrest (see Figure below from Lau’s paper attached below).
 Furthermore, the actual ICP can be estimated using the Gosling pulsatility index (PI). First, the PI can be calculated from the following formula.
Furthermore, the actual ICP can be estimated using the Gosling pulsatility index (PI). First, the PI can be calculated from the following formula.
Pulsatility index (PI) = (Peak systolic velocity – End diastolic velocity) / (Mean velocity)
From the PI (which machines with the TCD software package will give you automatically from tracing the spectral waveform) you can get the ICP through the following formula:
ICP = (10.93 x PI) – 1.28
In this case the PI was found to be 1.09. Therefore, using the above formula:
ICP = (10.93 x 1.09) – 1.28
=10.6 – essentially a normal ICP
Given the normal waveform and estimated ICP the parenchymal ICP monitor was thought to be non-functional. Neurosurgery was re-consulted and the ICP monitor was exchanged for an external ventricular drain (EVD) which showed a normal ICP of 10, corroborating our TCD results.
This case illustrates the utility of point-of-care TCD to help guide the management of the neurocritical care patient. See the attached article below by Lau & Arntfield detailing the use of point-of-care TCD by intensivists.
Click here: TCD
The Case
This is a 54 yo M who presented with acute hypoxic respiratory failure necessitating intubation and ICU admission. Post-intubation he had a P/F ratio of 54 despite a relatively unremarkable CXR. The PEEP was increased to try to improve oxygenation. A CTPA was ordered which was negative for PE and showed just a small right lower lobe consolidation. Given that the refractory hypoxia seemed discordant with the pulmonary pathology, concern was raised for an intracardiac shunt. A point-of-care TEE was performed including a bubble study. Have a look at the selected clips below and see what you think!


This is a positive bubble study for intracardiac shunt! To perform a bubble study using TEE the bicaval view is typically used. In this view you clearly see the LA, RA and interatrial septum. Injection of ~10cc of agitated saline allows easy visualization of a potential shunt. In this case, you can clearly see the immediate appearance of agitated saline in the LA after only 1-2 cardiac cycles. Interrogation of the interatrial septum further reveals an organized colour jet across what is likely a patent foramen ovale (PFO) and demonstrates the right to left shunt.
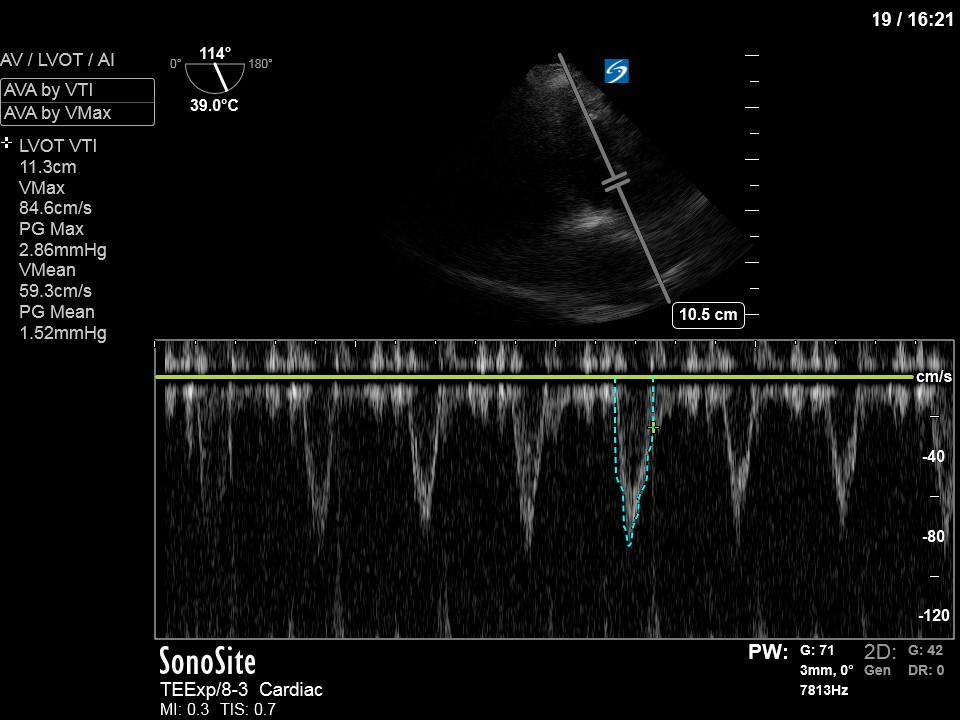
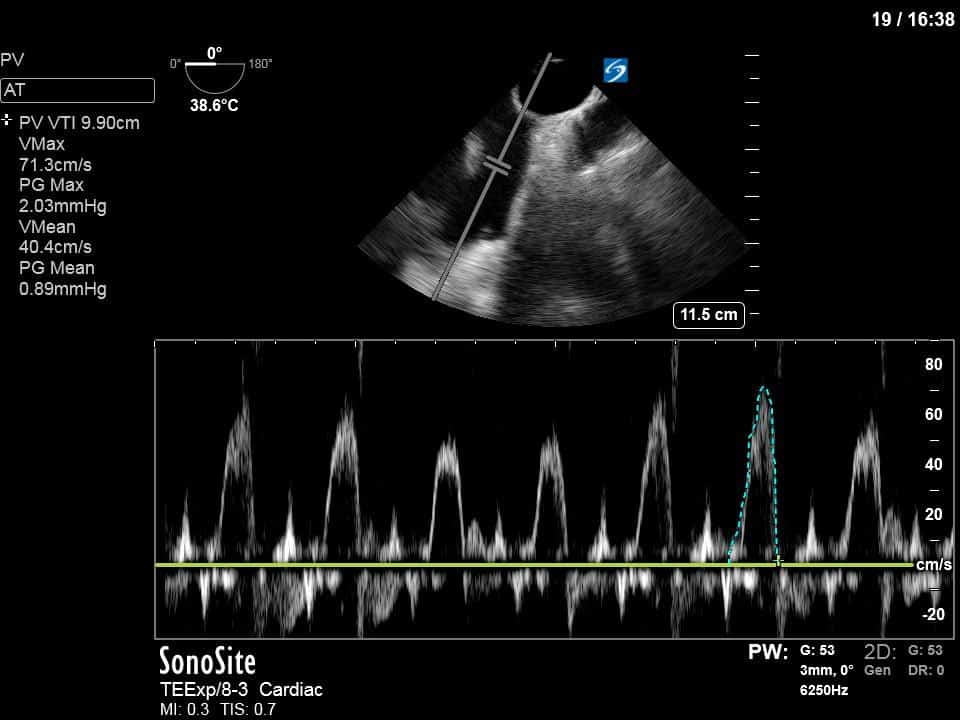
To further quantify the extent of the shunt, you can calculate the Qp:Qs – the ratio of right sided to systemic cardiac output. The calculation of Qs is the usual measurement of the LVOT VTI (see previous COTW or WesternSono screencasts for more information on this) and LVOTd to estimate the SV (and hence CO) of the LV. For Qp you apply the same principles but measure the RVOT VTI and RVOTd just before the pulmonic valve. This is best done in the mid-esophageal ascending aorta view which both gives a good view of the PV and main pulmonary artery and also allows an adequate insonating Doppler angle. In this specific case, we measured the VTI and measured the diameter in the main PA given that the RVOT was not adequately visualized in that view.
Doing the math in this case gives:
LVOT VTI = 11.4
HR 117
LVOTd = 1.93cm
CO (Qs) = (1.93/2) * VTI * 1.93
Qs = 3.9L/min
Main PA diameter = 1.84cm
Main PA VTI = 9.9cm
Qp = 3.1L/min
Qp:Qs = 3.1/3.9 = 0.8
A Qp:Qs of 0.8 essentially means that 20% of his CO is being shunted to the LV without being oxygenated by the lungs, likely greatly contributing to his refractory hypoxia. Thus, we recommended to decrease the PEEP (a counterintuitive move in hypoxia) to decrease the mean intrathoracic pressure and hopefully mitigate the right to left shunt.
Thanks for reading!
Matt
Hi everyone. It’s Matt back today, so you’ll have wait until next week for more EyeScandy!
The Case
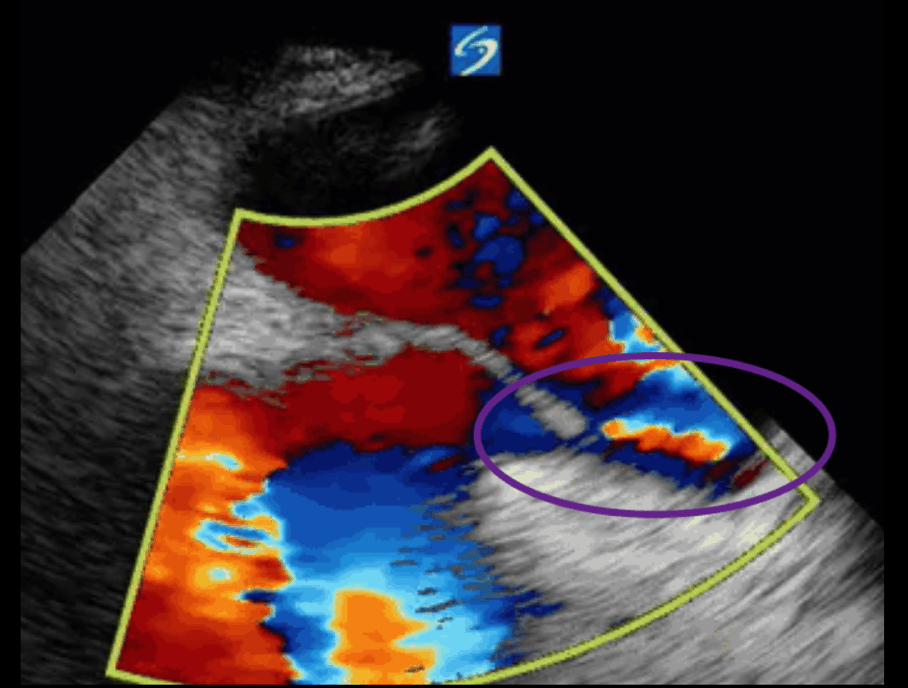
This is a case of a 56 yo F admitted with sepsis and MSSA bacteremia. A CT Head revealed several lesions concerning for septic emboli. She had known chronic significant mitral valve pathology documented prior to her admission. The POCUS team keen to see this pathology and to look for any additional signs of infective endocarditis. What do you notice about the valve on the 2D echo images and what specifically do you see on its colour doppler interrogation?
There is no clear definite lesion suggestive of endocarditis, but the images show a flail posterior mitral valve leaflet (PMVL) with associated severe MR. In the A4C view you can clearly see the abnormal mitral valve coaptation line, with the tip of the PMVL pointing towards the left atrium during systole (a hallmark finding of a flail leaflet). Colour doppler shows an eccentric, anteriorly directed MR jet.
Although, there was no obvious new vegetation on echocardiography (including a subsequent TEE) this patient met criteria (Duke criteria) for infective endocarditis. This is based on the patient fulfilling the major criteria of MSSA bacteremia, along with the presence her pre-existing MV pathology, fever, and evidence of septic emboli on her CT Head.
The flail leaflet had been documented previously secondary to myxomatous degeneration of the mitral valve apparatus with subsequent rupture of the chordae tendinae. The patient was actually awaiting open surgical repair of this valve, but unfortunately developed this illness prior to her operation. Overall, this case highlights a few important points about mitral regurgitation worth talking about.
First, is the general classification of mitral regurgitation. Mitral regurgitation can be classified as either primary or secondary. In primary MR the pathology is intrinsic to the valve itself. In contrast, secondary MR is a result of diseases of the LV (e.g. ischemic cardiomyopathy) and results from dilation of the MV annulus. The most common cause of primary MR is myxomatous degeneration causing mitral valve prolapse which can further progress to a flail leaflet, as seen in this case. Other causes of primary MR can include endocarditis, calcific leaflet degeneration and congenital abnormalities.
A variety of colour doppler, pulse wave doppler and continuous wave doppler techniques can be deployed to help grade the severity of MR. However, it is important to note that grading the severity of MR can be extremely difficult and nuanced, and as such, is often best left to the domain of formal echocardiography. In this case, the abnormal morphology of the MV (the flail leaflet) is consistent with severe MR, without necessarily having to apply more advanced Doppler techniques. Furthermore, the eccentric anteriorly directed jet is also a clue towards primary MV pathology, as secondary MR jets tend to be more central in nature.
The most important thing in this case would be to recognize the grossly abnormal 2D morphology of the MV and know to escalate this to a more detailed assessment. For those super keen on learning more about detailed MV assessment, you can check out the latest ASE guidelines on assessment of regurgitant lesions (attached below).
Emergency Medicine POCUS Series
Fundamentals
Abdominal Aorta
Abdomen
Female Pelvis
Cardiac
Your Content Goes Here
http://www.aesplin.com/tee-howtoscan/#Menu
Cardiac POCUS
Hi all,
I wanted to forward another free resource for your POCUS training. The folks at EGLS have made their course content available to all training residents. The content provides a pathway for the use of POCUS in unstable patients, and the fundamental teaching (ie cardiac conventions etc) is congruent with what you will experience on your TEAM POCUS rotations. If interested, they also have an app with their algorithm and some just in time learning. All of these links are available in your TEAM POCUS portal during your rotation.
Drew
1) EGLS Online is now available to Canadian EM residents for FREE!
https://edsonoshare.ca/egls-online-for-residents/
Websites
- Good Overview of all images/topics – Stanford
- Improving imaging tip – Angle for Center – Rotate for sides
- Toronto PIE – 3D simulator – FOCUS exam views as well as all other echo views
- https://criticalcarenorthampton.com/useful-echo-resources/
Pericardium
- Theory behind measuring effusions (website)
Other
- EPSS – article
- EPSS – US Podcast
PCE and Tamponade
- Slowly Crashing Patient in Tamponade (Mallemat) –
Thoracic
|
|
General Reference
Textbooks
Overviews of Thoracic US
US Podcasts (Matt and Mike)
Specific Topics
Protocols
References / Research |
Procedural
Renal
Gallbladder
General Reference
- LHSC Gallbladder Reference Document (required review)
- Sonosite Institute – Biliary Section (login:[email protected] pass:emlondon)
- Hartman’s Pouch and Phrygian Cap (image)
- Paucis Verbis Card – Focused Biliary US
- US Imaging of Biliary Tract (US Clinics) – Chapter
- US Leadership Academy – RUQ US – Overview (Blog)
Textbooks
- Point of Care Textbook (login:[email protected] pass:emlondon)
- Free iBook download Vol 1 and Vol 2 – Volume 2 – Chapter 15 – RUQ US
- Also available online (login:[email protected] pass:emlondon)
Narrated Lectures
- From Geoff Hayden (Emergencyultrasoundteaching.com) (38 mins)
- From Bret Nelson -SinaiEMUS (18 mins)
- South Carolina School Medicine – (11 mins)
- Sonosite – Gallbladder Overview (4:33)
- Sonosite – Phil Preyra – Part 1 Part 2 Part 3
- SoundBytes Cases – 2 parts
- CCUS – Mallemat (suboptimal quality) – Presentation
- Ultrasound Podcast – Gallbladder (24 mins)
Short Clips
- Ma and Mateer – Biliary – Normal (4:45)
- Ma and Mateer – Biliary – Abnormal (4:45)
- 5 Min Sono – Gallbladder
- 5 Min Sono – Gallbladder Pearls
Website Reading
- Ultrasound Leadership Academy – Overview
- Christian Fox – SonoGuide.com – Overview
- Phillips – Focused Ultrasound for Cholelithiasis – Online
- GB Adenomyomatosis – Hennepin – (Case)
- GB artifacts – Hennepin – (Case)
Specific Topics
- Common Bile Duct
- Where to measure (Twitter image)
References / Research
DVT
General Reference
- ACEP Imaging Compendium (required review)
- Key Scanning Zones (Image)
- Paucis Verbis Card – DVT
- Sonosite Institute – DVT Section (login:[email protected] pass:emlondon)
- US Leadership Academy – DVT US – Overview (Blog)
- Practical Ultrasound Series – DVT (Free iTunes ebook)
Textbooks
- Point of Care Textbook (login:[email protected] pass:emlondon)
- Free iBook download Vol 1 and Vol 2 – Chapter 4: Lung
- Also available online (login:[email protected] pass:emlondon)
Narrated Lectures
- From Geoff Hayden (Emergencyultrasoundteaching.com) (23 mins)
- From Bret Nelson -SinaiEMUS – (20 mins)
- Sonosite – DVT Study – (5:12)
- SoundBytes Cases –Part 1 (24 mins) Part 2 (20 mins)
- UltrasoundPodcast – How To – DVT (9 mins)
- UltrasoundPodcast – Approach to DVT (20 mins)
- UltrasoundPodcast – Controversy in 2 Point
- Ma and Mateer – DVT – How To (6 mins)
- DVT – Overview (18 mins)
- CastleFest – 2013 – Blaivas Lecture (25 mins) – PDF of Slides
Web Reading
- Online Ebook – Blaivas
- Ultrasound Leadership Academy – Overview
- Christian Fox – SonoGuide.com – Overview
- ACEP.org – Focus on DVT
Cases
- When is superficial not superficial (case)
References / Research